Abnormal Deliveries: Understanding Complications in Childbirth
Abnormal deliveries, also known as complicated or dystocic labors, occur when the natural progression of childbirth deviates from the expected course, leading to prolonged labor, increased risks, or the need for medical intervention. These situations affect a significant number of pregnancies and require prompt recognition and skilled management to ensure the safety of both mother and baby. While most deliveries proceed normally, abnormalities can arise due to issues with the “three Ps”: power (uterine contractions), passage (maternal pelvis), and passenger (fetus).
Causes of Abnormal Deliveries
Abnormal deliveries often stem from a combination of factors. Power-related issues include inadequate or irregular uterine contractions (hypotonic dysfunction), where the uterus fails to generate sufficient force to dilate the cervix or push the baby downward. This is common in primiparous women or after premature rupture of membranes.
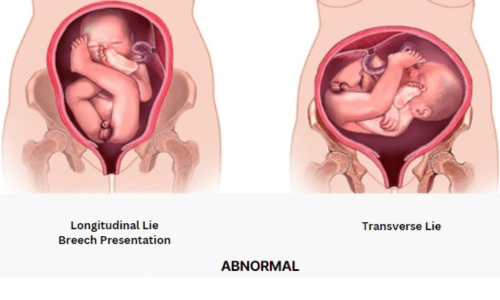
Passenger-related problems involve fetal factors such as macrosomia (large baby weighing over 4 kg), abnormal presentation (breech, transverse lie, or face/brow instead of vertex), or malpositions like occiput posterior. Shoulder dystocia, where the baby’s shoulders get stuck after the head delivers, is a critical emergency often linked to gestational diabetes or maternal obesity.
Passage-related causes include cephalopelvic disproportion (CPD), where the baby’s head is too large for the mother’s pelvic inlet, or soft tissue obstructions from fibroids, tumors, or edema. Additional contributors are maternal conditions like high blood pressure, infections (chorioamnionitis), or epidural analgesia, which can weaken contractions.
Types of Abnormal Deliveries
Common types include prolonged latent phase (slow initial cervical changes), active phase arrest (no progress despite strong contractions), and second-stage disorders (delayed descent or expulsion). Precipitous labor (extremely rapid delivery in under 3 hours) can cause trauma, while obstructed labor leads to mechanical blockage. Third-stage complications involve retained placenta or postpartum hemorrhage.
Management and Prevention
Early detection through regular antenatal check-ups, fetal monitoring, and partograph use is crucial. Management may involve augmentation with oxytocin for weak contractions, change in maternal position to correct malpresentation, or assisted delivery using vacuum/forceps. In severe cases like CPD, fetal distress, or shoulder dystocia, cesarean section becomes necessary to prevent maternal exhaustion, infection, or fetal hypoxia.
Specialized obstetricians emphasize evidence-based care, including promotion of vaginal births where safe, while preparing for interventions in high-risk cases. With multidisciplinary support, most abnormal deliveries result in healthy outcomes.